What Are My Gynecomastia Surgery Options?
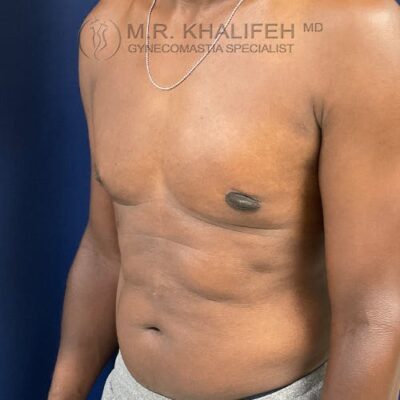
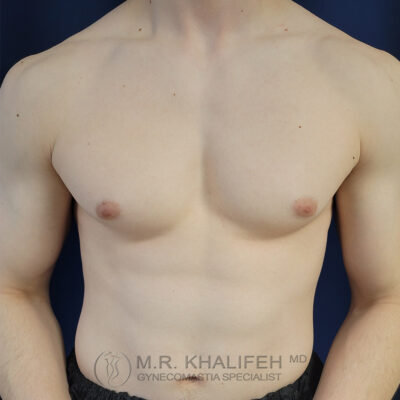
In an ideal setting any gynecomastia surgery will be to get you a flat chest, avoid too much scarring, avoid skin overhang, and correct nipple position issues and sizes.
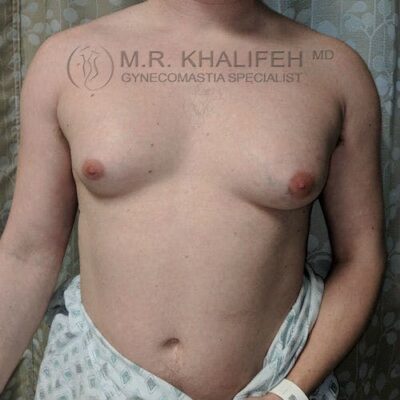
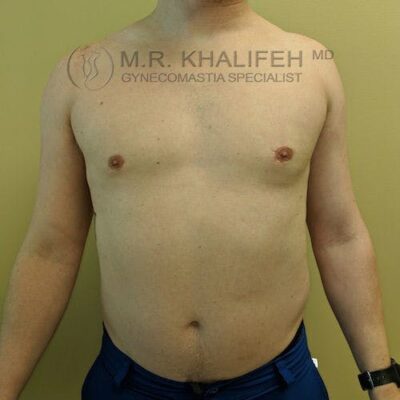
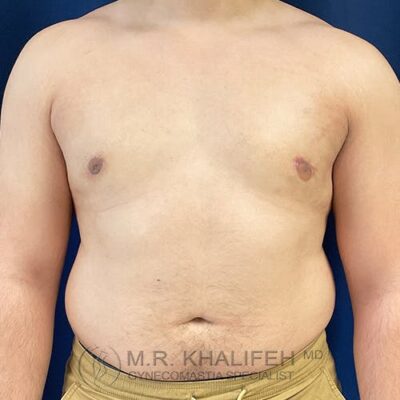
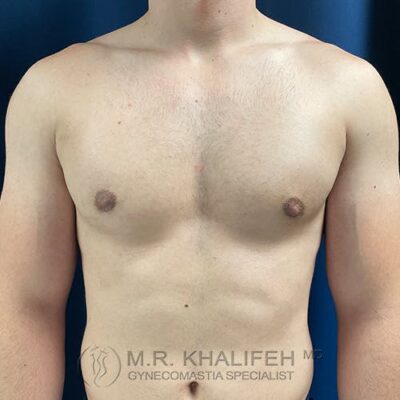
To get to a flat chest, direct gland excision is the mainstay, often combined with a certain amount of lipo. The amount of lipo correlated with the amount of excess fat both in the breast and in the lateral chest and axilla. For example in the subset we term “puffy nipple”, we rely almost exclusively on the gland excision, whereas in the subset we refer to as “pseudogynecomastia” we rely mostly on the liposuction part of the case.
The least visible scar is on the inferior aspect of the nipple-Areola. The vast majority of my surgical cases (80%) involve me working through the lower third of the nipple to extract the fat and gland, leaving very little scarring.
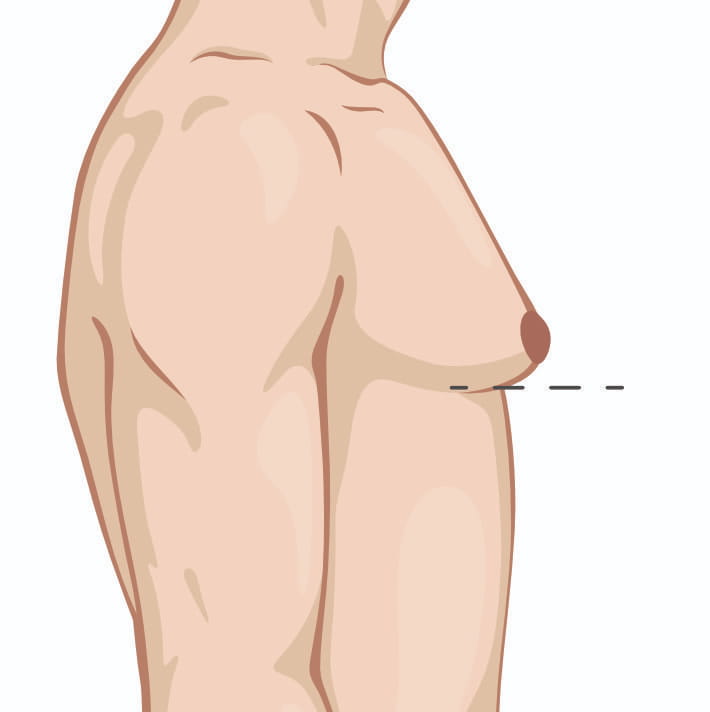
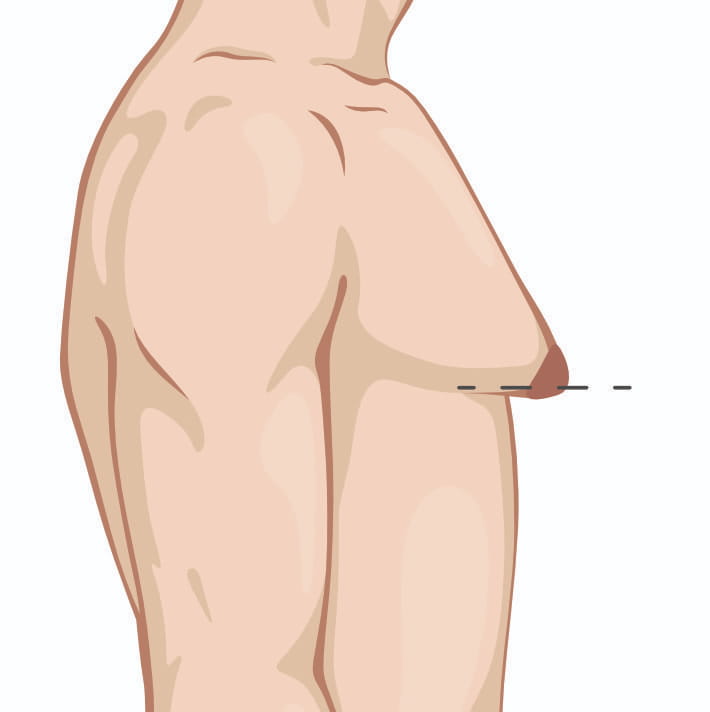
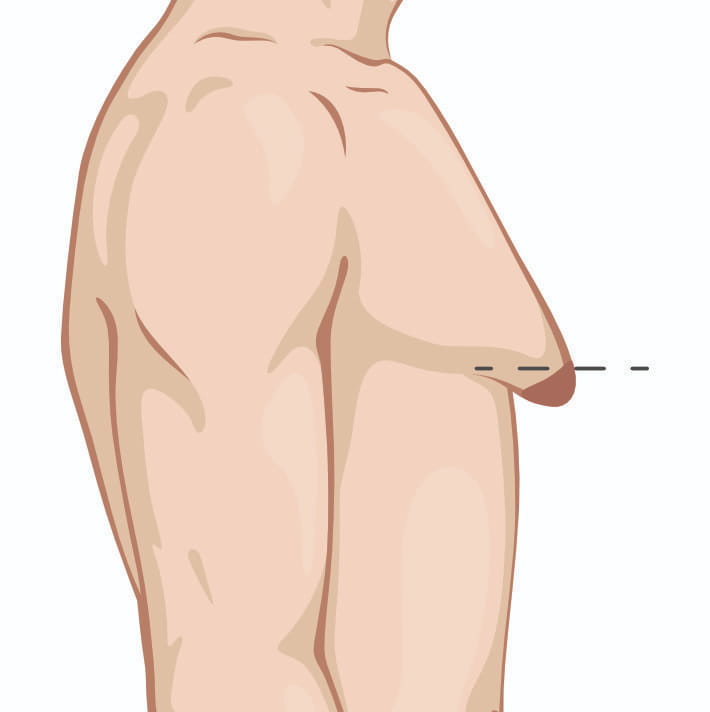
Once you have skin excess or enlarged/malpositioned nipples, I will have to discuss with you the option of doing additional maneuvers to address those issues. Those options include removing an ellipse of skin (downside is a chest scar) or removing some skin around the nipple and changing the size /position of the nipple (downside is a scar all round the nipple). These maneuvers become more needed as the grade in severity of gynecomastia progresses.
Finally, a word on anesthesia. I perform the vast majority of cases (90%) in an office setting using local anesthesia with mild oral sedation. In some cases, due to either extent of planned surgery or patient preference, the surgery is performed under general anesthesia in a hospital setting.